









Patrick Bellgowan, PhD, Deputy Associate Director, NINDS
Dr. Bellgowan shared an overview of TBI, including the causes of injury, categorized as blunt force, blast exposure, and penetrating injury. The factors impacting TBI are complex and interrelated, and include severity of injury, age, gender, injury type, history of prior TBI, genetics, and social determinants of health. Understanding the diagnostics and treatment of TBI is an evolving landscape. One of the issues facing experts is how to define and categorize TBI. The National Institutes of Health (NIH) are investing across the research spectrum with at least 11 of the institutes involved in the TBI portfolio. NINDS leads this work within NIH. Dr. Bellgowan shared that while federal agencies historically worked in silos on this issue, a 2012 Executive Order established the National Research Action Plan (NRAP), asking all federal agencies to work together to improve access to mental health services for veterans, service members, and military families. An interagency task force was established to implement the order and the Department of Health and Human Services (HHS), the Department of Veterans Affairs (VA), and the Department of Defense (DOD) have since coordinated efforts to combat TBI.
Dr. Ramoni followed and shared how the VA is contributing to the NRAP, first noting that to accelerate progress in TBI diagnosis and treatment we must build on the NRAP to more precisely diagnose sub-types of TBI that are similar in their types and length of symptoms and respond to the same treatments. An important path toward progress is to leverage data that already exists. The VA has data in their electronic health records dating back to 1999, which includes complete medical record information on 16.6 million veterans and partial information on another 10 million veterans. Additionally, the Million Veterans Program, a national research program to discover how genes, lifestyle, and military exposures affect health and illness, has data on over 830,000 veteran volunteers. The VA is working to establish a VA Data Commons in collaboration with the University of Chicago and the Open Commons Consortium. This will allow approved VA and non-VA researchers to access de-identified data from VA’s electronic health records. A pilot is expected to launch in 2022.
Rachel B. Ramoni, DMD, ScD, Chief Research & Development Officer, U.S. Department of Veterans Affairs

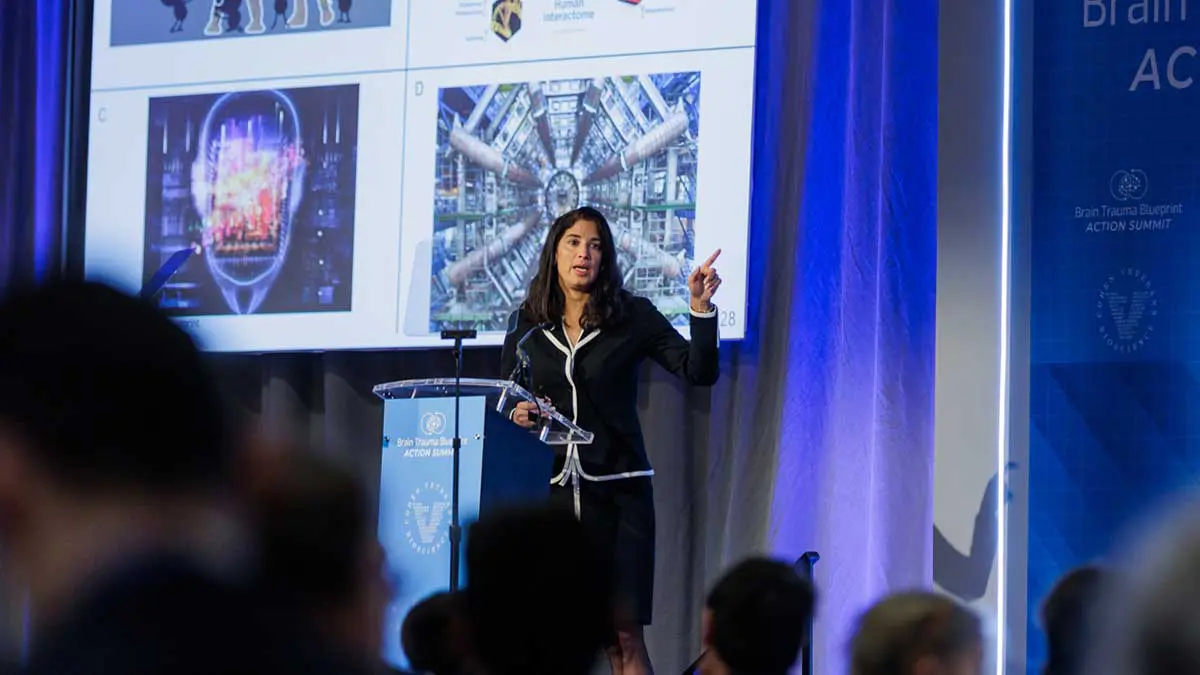
Magali Haas, MD, PhD, CEO & President, Cohen Veterans Bioscience
Next Dr. Haas discussed CVB’s mission to advance brain health by advancing precision medicine solutions. Dr. Haas shared an update on the Brain Trauma Blueprint, a roadmap to advance a first generation of targeted solutions for TBI, focusing on the chronic sequelae. The Brain Trauma Blueprint is born from the recognition that there are currently no FDA-approved therapies for TBI, and was the basis for the 2019 State of the Science Summit on TBI, which brought together over 100 thought leaders across the research ecosystem to identify the research gaps that have stymied progress as well as specific recommendations to overcome these gaps through a consensus research roadmap. The specific recommendations are to be published as part of a six part publication series in the Journal of Neurotrauma. If these efforts to align resources toward these gaps and priorities is successful, it will help catalyze a first generation of targeted treatments for TBI. The Brain Trauma Blueprint has already led to new public-private partnerships and collaborations, many of which were described in this briefing. Dr. Haas outlined some of the most pressing needs identified through the Brain Trauma Blueprint, including the need for a national surveillance system for all severities of TBI. At this time, the United States does not have a reliable method for tracking TBI; rather, it only tracks individuals affected by TBI based on emergency room encounters. It is important that a national surveillance system to track the number of individuals who sustain TBI, including those who do not seek care in an emergency setting.
Dr. Stone discussed his work toward developing a Normative Neuroimaging Library, supported by CVB. The field of neuroimaging is more than 100 years old. Since that time there has been significant expansion of capabilities around neuroimaging, but the ability to be able to pull information from the images and the clinical processes to interpret the images and manage care have remained relatively static. Current approaches are helpful for moderate to severe TBI where routine neuroimaging exams can reveal urgent findings. However, routine neuroimaging approaches have a relatively limited role in mild TBI and concussion, which constitute the vast majority of TBI seen in the U.S. In recent years, there have been advanced neuroimaging techniques that have allowed us to push the boundaries in what we can see, but these approaches require the acquisition of a large volume of images and require computational tools to derive certain measures. A Normative Neuroimaging Library will provide the foundational building blocks to bridge the gap between research and clinical applications for advanced neuroimaging and will address the rapidly expanding need for quantitative, diagnostic neuroimaging tools.

James R. Stone, MD, PhD, Associate Professor, Radiology & Medical Imaging, University of Virginia School of Medicine

Jamshid Ghajar, MD, PhD, President, Brain Trauma Foundation, Director, Stanford Brain Performance Center
The final speaker on the panel, Dr. Ghajar, discussed the Brain Trauma Blueprint and the impact of evidence-based solutions for diagnostics and treatment on coma, or severe TBI. Prior to the year 2000, there were no evidence-based guidelines in
place for individuals with severe TBI. Patients received very little brain pressure monitoring, were given steroids, were under-resuscitated and mortality was 50%. The Brain Trauma Foundation (BTF) created 21st century evidence-based guidelines calling for brain pressure monitoring, no steroids, no hyperventilation, full resuscitation and full feeding. As compliance with the guidelines went up, mortality went down, dropping to 25%. The CDC issued a report on the impact
of the BTF guidelines and similarly found a 50% decrease in death as well as
cost savings. Now the guidelines, which are constantly updated, are used in
every trauma center in the U.S. as well as internationally. The BTF continues to establish and update evidence-based guidelines for different areas including hospitals, ambulance care and the military. With the Brain Trauma Blueprint, there is a roadmap to move forward with further evidence-based solutions.
Dr. Matthew Rizzo, Chair of the American Brain Coalition, closed the briefing by encouraging Members of Congress to join the Congressional Neuroscience Caucus and Congressional Brain Injury Task Force and asked congressional staffers in the audience to support federal funding for biomedical research, including brain injury research.
About the Brain Trauma Blueprint
The Brain Trauma Blueprint is a framework to advance precision diagnostics and therapeutics for brain trauma through a process of community stakeholder consensus roadmapping and collaborative execution. More information can be found here.